14. Asthma Management in the PICU
Asthma Clinical Practice Guidelines
Status Asthmaticus
Defined as a condition of progressively worsening bronchospasm and respiratory dysfunction caused by asthma. When unresponsive to standard conventional therapy, it may progress to respiratory failure, the need for mechanical ventilation, extracorporeal support, and even death. Children with status asthmaticus have the highest need for support from our pediatric intensive care unit (PICU).
Criteria for PICU Admission
- Prolonged continuous albuterol for > 4 hours with worsening symptoms
- Inadequate ventilation with hypercapnia (pCO2 on capillary gas >45)
- Need for high flow nasal cannula (> 0.25L/kg/min or >10L or >40% FiO2) or non-invasive ventilation
- Persistent hypoxemia (SpO2 <90%) despite supplemental O2 (≥3L/min or >40% FiO2 with non-rebreather)
- Altered level of consciousness (drowsiness)
Transfer to a higher level of care is recommended if there is a concern for impending or actual respiratory arrest. The progression from respiratory distress to respiratory failure to respiratory arrest can vary by patient. Respiratory failure can progress rapidly and be difficult to reverse. Therefore, it is important to emphasize the signs of impending respiratory arrest.
Signs of Respiratory Arrest
- Altered level of consciousness (LOC) – this may manifest as drowsiness or sleepiness in young children. Hypoxemic seizures or syncope can also be a complication to status asthmaticus.
- No improvement after magnesium sulfate administration in conjunction with continuous albuterol.
- Pediatric Early Warning Systems (PEWS) score of 6 or CMH Respiratory Care Score of greater than 9 without improvement.
- Oxygen requirement greater than 40% FiO2
- Hypoventilation – may develop more rapidly in young children
- Hypercapnia – Monitoring CO2 levels is a useful indicator of impending failure Arterial blood gas with PCO2>42 is associated with high risk of impending respiratory arrest in acute situations.
- Paradoxical thoracoabdominal movement (See-saw breathing)
- Absence of wheezing – when airway obstruction is so severe that no air can be auscultated. This can be especially difficult to detect for novice health care providers; hence, auscultatory findings should be considered in clinical context.
- Bradycardia – heart rate changing from tachycardia to bradycardia
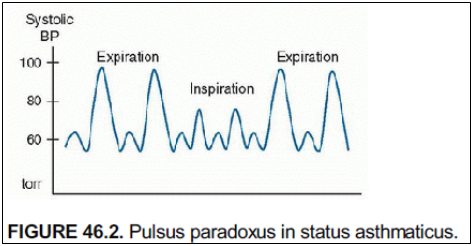
- Resolution of prior pulsus paradoxus – in the absence of improving respiratory status, resolution of pulsus paradoxus can suggest respiratory muscle fatigue.
Basic Pathophysiology of Asthma Exacerbation
Lower airway obstruction due to:
- Bronchial smooth muscle contraction (bronchoconstriction)
- Increased mucus production leading to mucus plugging
- Airway inflammation and edema
Cardiopulmonary interactions
- Hyperinflation of the lungs leads to increased pulmonary vascular resistance. This then leads to increased right ventricle afterload with subsequent decreased right ventricular function.
- High intrathoracic pressure from hyperexpanded lungs leads to decreased venous return to the heart, thereby decreasing preload and subsequently cardiac output.
Evaluation
History
- Asthma severity
- History of consultation from allergy/immunology or pulmonology
- Medication adherence
- Previous ED/UCC visits or oral steroid courses in the last 12 months
- Previous hospitalizations
- Previous ICU admissions
- Previous need for non-invasive ventilation (e.g. BiPAP), intubation and mechanical ventilations or extracorporeal membrane oxygenation (ECMO)
- Triggers, specifically for this admission
- Signs/symptoms of concomitant viral or bacterial infection
Physical Exam
- Vitals
- Respiratory Rate and oxygen saturation at minimum, but a full set of vitals is important to assess patient’s status
- Albuterol can cause temporary V/Q mismatching resulting in mild hypoxemia
- Pulsus paradoxus – large negative intrathoracic pressure during inspiration leads to increased left ventricle afterload which manifests as decreased systolic blood pressure.
- Auscultation
- Typically, children will have a prolonged expiratory phase with asthma. Wheezing can be inspiratory, expiratory, or both (biphasic) but is from the lower airway and classically a polyphonic noise.
- Quality of air movement – lack of wheezing combined with poor air movement is very concerning!
- Work of breathing
- Evaluate typical signs of respiratory distress – retractions, grunting, nasal flaring, head bobbing.
- Distress may be more subtle in older children/teens or in patients with a history of severe baseline obstructive lung disease.
- Can they speak in complete sentences? Or only short phrases? One word at a time?
Imaging and Laboratory Evaluation
- Chest X-Ray
- Often hyperinflated with flattened diaphragms due to air trapping
- Narrow cardiac silhouette due to high intrathoracic pressure
- Evaluate for signs of viral or bacterial infection
- Look for signs of air leak: subcutaneous air, pneumomediastinum, pneumothorax.
- Lab Results
- Complete Blood Count with Differential
- Electrolytes
- Consider infectious workup
- Consider blood gas
Treatment Options
Continuous Albuterol
- Dosed at 10, 15, or 20mg/hour
- Can be administered via:
- Large volume nebulizer and aerosol mask
- High Flow Nasal Cannula
- Best deposition at flows of 0.25L/min/kg
- Higher flows may decrease deposition and effectiveness
- Non-invasive Ventilation
- Mechanical Ventilation
- Mechanism: beta 2 receptor agonist leading to smooth muscle
- Side effects
- Tachycardia
- Agitation/Hyperactivity
- Tremors/Jitteriness
- Dysrhythmias
- Hyperglycemia
- Hypokalemia
- Diastolic hypotension with subsequent ECG changes
- Elevated troponin levels
- CMH caveat: Nebulized bronchodilator solutions in the United States can include preservative products that cause bronchospasm. These preservative products are sulfites, benzalkonium chloride (BAC), and chlorobutanol. In particular, BAC can lead to bronchoconstriction; this bronchoconstriction is cumulative, prolonged, and correlates with airway hyperresponsiveness. At CMH, we do not use BAC containing products, but these can be used at outside institutions and contribute to unresponsive bronchoconstriction.
IV Corticosteroids
- All asthma patients admitted to the PICU should receive IV corticosteroids
- Mechanism: suppress cytokine production and inflammation
- IV Solumedrol (methylprednisolone) – high glucocorticoid effect and minimal mineralocorticoid effect
- Dose: 2mg/kg load + 0.5-1mg/kg Q6 hour
- Side effects:
- Hyperglycemia
- Hypertension
- Agitation
IV Magnesium Sulfate
- Mechanism: smooth muscle relaxation
- Dose: 25-50mg/kg IV over 30-60 minutes or drip at 10-20mg/kg/hr
- Often given in conjunction with a small fluid bolus as it can cause hypotension
- Side effects:
- Hypotension
- Central nervous system depression
- Flushing
Ipratropium bromide (Atrovent)
- Mechanism: anticholinergic that impairs smooth muscle contraction
- Dose:
- 1500mcg combined with first hour of continuous albuterol
- 125-500mcg neb or 4-8 puffs Q4-8 hours
- DuoNeb = 2.5mg albuterol + 500mcg Atrovent combined
- CMH does not have DuoNeb on formulary. Albuterol and Atrovent must be ordered separately and RT will combine for treatment.
- Side effects:
- Dry mouth
- Flushing
- Tachycardia
Subcutaneous or Intramuscular Epinephrine
- Can be given in Emergency Department or enroute or PICU when air movement is so poor that inhaled bronchodilators are ineffective.
- Mechanism: stimulate all adrenergic receptors (alpha, beta1, beta2). Beta2 agonism leads to bronchodilation.
- Dose: 0.01 mg/kg up to a max of 0.5mg. May be repeated 1-2 times every 20 minutes.
- Most home epinephrine pens are dosed at 0.15mg for 15-30kg patient or 0.3mg for >30kg patient.
- Risks
- Lack of control over the dose especially if using a standardized epinephrine pen
- Difficult to “down-titrate” for complications
- Side effects:
- Arrythmia
- Cardiomyopathy
- Glucose changes
- Hypokalemia
- Tissue necrosis at site
- Jitteriness/Shakiness
- Headache
- Nausea
- Excessive doses can cause constriction of skeletal and vascular smooth muscle
Terbutaline
- Intravenous formulation makes it useful if air movement is so poor that inhaled bronchodilators are not effective
- Mechanism: Beta2 receptor agonist leads to bronchial smooth muscle relaxation with less effect on heart rate
- Dose:
- IV: 10mcg/kg load + drip at 0.1-10mcg/kg/min
- SubQ: 0.01mg/kg Q15-20 minutes x 3
- Side effects:
- Tachycardia
- Diastolic hypotension
- Dysrhythmias
- Nervousness
- Decreased serum potassium
- Increased serum glucose
- Tremor
- Not commonly used at CMH
Aminophylline
- Mechanism: methylxanthine derivative. Non-selective phosphodiesterase (PDE) inhibition that leads to bronchodilation and inflammatory downregulation
- Dose: 5-7mg/kg load + drip at 0.5-0.9mg/kg/hour
- Serum concentrations must be checked. Goal level 10-20 (very narrow therapeutic window)
- Side effects:
- Nausea/vomiting
- Tachycardia
- Hypotension
- Irritability
- Seizures or arrhythmia can occur with high levels (>35)
Ketamine
- Mechanism: bronchodilation via multiple potential mechanisms – immunomodulation, catecholamine upregulation, decreased nitric oxide, anticholinergic effects
- Dose: continuous drip at 0.5-1mg/kg/hour
- Often used for sedation when intubating an asthmatic
- Intubation sedation dose: 1-2mg/kg
Respiratory Support in PICU
Heliox
- Mixture of helium and oxygen gas with a density less than room air.
- Mechanism: improves laminar flow, may improve distribution and deposition of nebulized medications. Leads to decreased work of breathing for disorders characterized by airway resistance.
- Tanks are available in 80:20 (80% helium, 20% oxygen mixture)
- If patients need increased FiO2, this can be bled into the system, but helium becomes non-therapeutic with FiO2 greater than 40%
- There is controversy regarding use in acute asthma exacerbations with some studies finding benefit and others that found none.
- Heliox does NOT replace bronchodilation and corticosteroid therapy and should only be considered as adjunctive care.
- Can only be delivered in ED or PICU
Inhaled Anesthetics (Isoflurane, Sevoflurane)
- Administered only by anesthesia in room with a scavenger system and specialized ventilator (i.e. OR). Risks of use in PICU without a scavenger system includes difficulty monitoring, volatility of gas, and impact on health care providers.
- Administered in intubated/mechanically ventilated patients with life threatening bronchospasm
- Mechanism: bronchodilation via multiple mechanisms
- Side effects:
- Sedation
- Hypotension
- Dysrhythmia
- Not currently available at CMH
Mechanical Ventilation
- Indications:
- Respiratory failure with profound hypercarbia/acidosis
- Decreased mental status
- Severe refractory hypoxia
- There is a high risk for cardiac arrest during intubation
- High intrathoracic pressure leads to decreased preload with subsequent decreased cardiac output and hypotension. This worsens when you add invasive positive pressure which adds to right heart afterload and decreases forward blood flow.
- Anticipate hypotension and give volume!
- Risks:
- Worsening bronchospasm
- Ventilator induced lung injury, especially barotrauma and volutrauma
- Air leak, pneumothorax, pneumomediastinum
- Hypotension due to decreased preload
- Infection
- Cardiac Arrest
Ventilator Management
- Low respiratory rate and long expiratory time (I:E of 1:4 or 1:5)
- Low tidal volume (5-6mL/kg)
- Low peak pressures (PIP) (alveolar pressure and pressure due to airway resistance)
- Measure and trend plateau pressures (Pplat) (the pressure the alveoli see)
- Typically, intubated asthmatics will have a large gap (>5) between PIP and Pplat
- Allow for permissive hypercapnia
- Monitor for auto PEEP (alveolar air trapping)
- Make sure measured PEEP (total PEEP) is not higher than PEEP by performing an expiratory hold
- Total PEEP – set PEEP = Auto PEEP
- Increasing set PEEP may seem counterintuitive, but may assist with decreasing auto PEEP
- Avoid paralysis
Ventilator Wave Forms
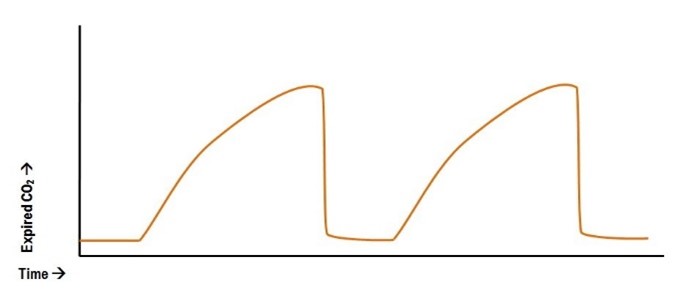
- May see “ramping” of end-tidal due to bronchospasm.
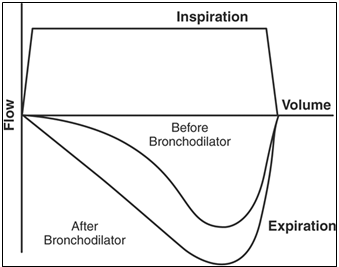
Flow patterns on ventilator can also show scooping on expiratory phase with improvements after bronchodilator.
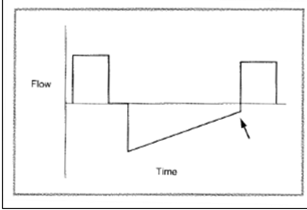
Flow patterns on a ventilator may also show air trapping as the expiratory flow limb does not return to baseline indicating ongoing air trapping.
Extracorporeal Membrane Oxygenation (ECMO)
- A full discussion on ECMO is outside the scope of this reference guide
- Indications for ECMO for an asthma exacerbation:
- Worsening hypoxemia despite maximal support or mechanical ventilation
- Worsening air leak
- Worsening acidosis (respiratory or metabolic)
- It is important to continue asthma management (i.e. steroids, albuterol, etc.) while on ECMO. Consideration for extubating while on ECMO can also be made once the patient is stable.
High Risk Asthma Protocol (HRAP)
Patients qualify for HRAP if:
- ≥ 4 acute care visits (ED, Urgent Care, or admission) in the 12 months OR were admitted to the PICU for asthma
Identification of these patients prior to discharge allows for appropriate follow-up but also helps providers know which patients are at greater risk to return for asthma care.
Use the High-Risk Asthma Order-set instead of the Inpatient Asthma Pathway Order-set. The High-Risk Asthma Order-set includes:
- Consult to Allergy or Pulmonology subspecialty groups for long-term care
- Consultation to Pulmonary Medicine should be done if patient has been seen in outpatient Pulmonary clinic in the past 2 years.
- Consultation to Allergy & Immunology Medicine should be done if patient has been seen in the Allergy and Immunology Clinic in the past 2 years.
- If the patient has not been seen by either specialty team, consultation per PICU attending preference.
- For patients with food allergy along with asthma, please consult Allergy/Immunology for comprehensive management of both.
- Social Work Consult
- Environmental Health Home Assessment Referral
AAIR Clinic Patients
Patients followed in the AAIR Clinic have severe refractory asthma and may have small airways dysfunction at baseline. These patients may not manifest typical signs of respiratory distress. Therefore, the AAIR patient policy should be followed:
- Respiratory Care Scores may not be an accurate representation of the level of distress.
- Beta-agonists should be ordered as scheduled treatments rather than per standard Respiratory Care Plan protocol.
- AAIR Clinic patients should receive a Pulmonary consult.
- Beta-agonists should remain at least Q2 until the patient is assessed by pulmonary medicine or discussed with pulmonary medicine/AAIR clinic provider by phone.
- Beta-agonist spacing should be decided as a group through frequent reassessment by inpatient medical staff, RT, and pulmonary consult.
Recommended Reading
- Fuhrman & Zimmerman’s Pediatric Critical Care, 5th Ed. Chapter 53: Asthma.
- Rogers’ Textbook of Pediatric Intensive Care, 5th Edition. Chapter 47: Acute Severe Asthma.
- Asthma Reference Guide Home
- 1. Introduction to Asthma
- 2. Asthma Diagnosis
- 3. Asthma Presentation
- 4. Goals of Asthma Therapy and Management
- 5. Asthma Severity and Asthma Control
- 6. Asthma Outpatient Management
- 7. Treating Modifiable Risk Factors
- 8. Treating Co-Morbid Conditions
- 9. Asthma Medications
- 10. Yellow Zone Therapy Options
- 11. Allergy Immunotherapy and Biologic Therapy
- 12. Asthma Exacerbations in the Emergency Department or Urgent Care
- 13. Special Asthma Considerations for Inpatient
- 14. Asthma Management in the PICU
- 15. Respiratory Support for Asthma Exacerbation
- 16. Asthma Education Resources