12. Asthma Exacerbations in the Emergency Department or Urgent Care
Asthma exacerbations
Asthma exacerbations are a common cause of respiratory distress. When evaluating a patient with respiratory distress thought to be secondary to asthma, a brief history and physical examination should be conducted concurrently with the prompt initiation of therapy.
Asthma Clinical Practice Guidelines
History
- Timing of onset
- Trigger (if known)
- All current controller and reliever medications including doses, devices, adherence pattern, recent changes, frequency during current exacerbation, timing of last doses, and perceived response to therapy
- Risk factors associated with increased risk of asthma-related death (Box 9-1 GINA 2025)
Box 4-1. Factors that increase the risk of asthma-related death
-
A history of near-fatal asthma requiring intubation and mechanical ventilation⁷⁴²
-
Hospitalization⁷⁴²˒⁷⁴³ or emergency care visit for asthma in the past year
-
Currently using or having recently stopped using oral corticosteroids (a marker of event severity)⁹⁵˒⁷⁴²
-
Not currently using inhaled corticosteroids⁹⁶˒⁷⁴²
-
Over-use of short-acting beta₂-agonists (SABA), especially use of an average of more than one canister of salbutamol (or equivalent) per month,⁹³˒¹¹⁷˒⁷⁴⁴ or using nebulized SABA⁷⁴⁵
-
Poor adherence to ICS‑containing medications and/or poor adherence to (or lack of) a written asthma action plan¹⁰⁹
-
A history of psychiatric disease or psychosocial problems¹⁰⁹
- Food allergy in a patient with asthma⁵⁵⁴˒⁷⁴⁶
-
Certain comorbidities, including pneumonia, diabetes, and arrhythmias (independently associated with an increased risk of death after hospitalization for an asthma exacerbation)⁷⁴³
Physical Exam
The severity of asthma exacerbations can range from mild distress to respiratory failure. There are several objective respiratory screening tools available to help assess the severity of respiratory distress. However, of the studies reviewed by Children’s Mercy Department of Evidence Based Practice in June 2020, none had been studied outside of the institution that developed them. It is unknown if the scores are transferable to other settings. When there is a lack of scientific evidence, standard work should be developed, implemented, and monitored.
- Previously, the Children’s Mercy ED used the Pediatric Respiratory Assessment Measure (PRAM) to determine asthma severity upon presentation and guide decision making on nurse-initiated orders. However, in an effort to be more consistent throughout the institution, the Pediatric Asthma Score (PAS) is now recommended to be used to assess severity of an asthma exacerbation.
- The Pediatric Asthma Score (PAS) is a validated scoring tool to provide an objective measure of asthma severity. It uses five assessments to classify respiratory distress due to asthma as mild, moderate, or severe. When combined with a clinical treatment protocol, the PAS has been shown to reliably decrease the length of stay, reduce cost related to asthma management, and improve quality of care for children with asthma.1
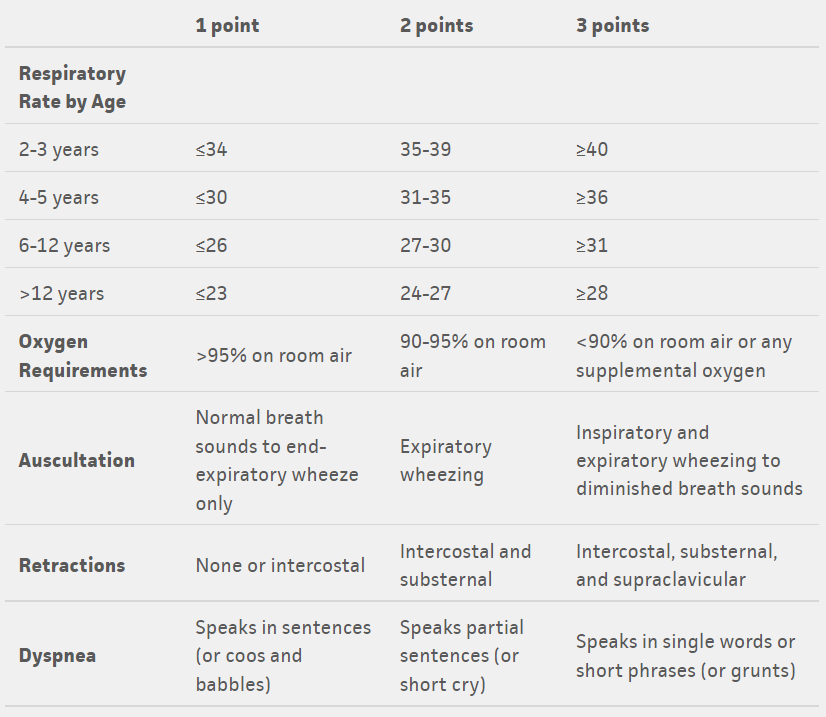
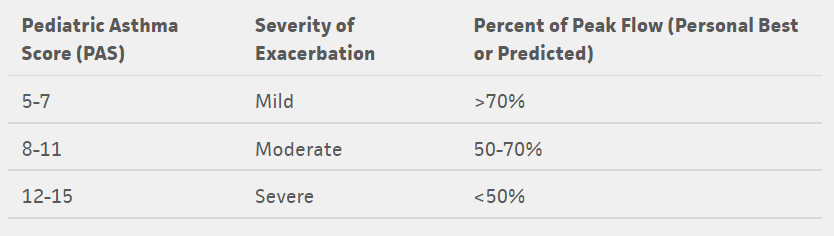
Tables from: https://www.mdcalc.com/pediatric-asthma-score-pas
Treatment
Children’s Mercy has developed clinical pathways for the evaluation and management of asthma exacerbations by location as different locations have access to different resources and can care for patients at different levels of acuity. The Asthma Care Continuum considers patients with asthma in 4 different locations within our health system emphasizing the need for similar language and treatment as a patient progresses through the continuum.
Asthma Clinical Practice Guidelines
Special considerations for urgent care
Magnesium Sulfate - because of many factors including the high acuity of patients requiring IV magnesium sulfate, and the risk of hypotension associated with administration of magnesium sulfate in a geographically isolated facility, IV magnesium sulfate is not available at Children’s Mercy Urgent Cares.
Continuous Albuterol - due to the ability to staff respiratory therapists in urgent cares, continuous albuterol is not available. Three back-to-back albuterol treatments with ipratropium is similar in dosing to one hour of continuous albuterol.
- If the patient is significantly improved after 3 back-to-back doses of albuterol where discharge home is likely after a period of observation, the patient can continue to be managed in the urgent care.
- If the patient is improving but may benefit from additional treatments not available (i.e. magnesium sulfate), consider transfer to the ED.
- If the patient is minimally improved, consider admission via transport.
Special Considerations for Steroid Administration
Corticosteroids PO or IV (if not tolerating PO) should be administered within one hour of arrival for patients with an asthma exacerbation so they have time to take effect. Patients given steroids within the first hour of presentation were significantly less likely to be admitted to the hospital.2
- Short courses of corticosteroids are associated with fewer relapses to additional care, fewer hospitalizations, and less need for beta agonists.
- Literature shows that 1-2 days of dexamethasone (0.6mg/kg/day) have been shown to be equivalent to 5 days of prednisone (1-2mg/kg/day).3-5
- Dexamethasone is therefore listed as the preferred systemic steroid for mild to moderate exacerbations in the ED/UCC as it can be administered in a single dose without the need for families to obtain refills of medications after discharge home.
- Severe exacerbations should be treated with IV methylprednisolone as it may be unsafe for patients to take oral medications.
Disposition to Home
After treatment and a period of observation in the ED or Urgent Care, if the patient’s symptoms are resolving, the patient is no longer in respiratory distress, and the family is comfortable continuing care at home, they may be discharged from the ED.
- Review asthma action plan with family (this can be done by the respiratory therapist via the order “RT Education” within the ED asthma power plan).
- Ensure patient has sufficient supply of controller and/or rescue asthma medications, as well as a prescription for the complete course of systemic steroids if indicated.
- If the patient is not on a controller medication, consider starting one appropriate for patient’s asthma severity. See Stepwise Approach
- Ensure follow up within one week with a provider, preferably primary asthma provider if available or PCP if unavailable.
Disposition to Inpatient
If patient’s symptoms are not improving despite interventions or are requiring supplemental oxygen therapy, they should be admitted to the hospital for further management.
- Patients followed in the AAIR Clinic (as indicated by a critical information note) have severe refractory asthma and may have small airways dysfunction at baseline. These patients may not manifest typical signs of respiratory distress. Therefore:
- PAS scores may not be an accurate representation of the level of respiratory distress.
- AAIR Clinic patients should receive a Pulmonary consult.
- Beta-agonists should remain at least Q2 until the patient is assessed by pulmonary medicine or discussed with pulmonary medicine/AAIR Clinic provider by phone.
- All other patients can be admitted to general pediatrics.
- If there is a delay in going up to the inpatient unit, please ensure the patient continues to receive albuterol therapy at minimum every 2 hours as indicated.
Criteria for PICU admission
- Prolonged continuous albuterol for > 4 hours with worsening symptoms
- Inadequate ventilation with hypercapnia (pCO2 on capillary gas >45)
- Need for high flow nasal cannula (> 0.25L/kg/min or >10L or >40% FiO2) or non-invasive ventilation
- Persistent hypoxemia (SpO2 <90%) despite supplemental O2 (≥3L/min or >40% FiO2 with non-rebreather)
- Altered level of consciousness (drowsiness)
If there is a delay in going up to the PICU, please ensure that patient continues to receive albuterol therapy as indicated.
Contacting Subspecialists
If the patient and/or family identifies a physician as their primary asthma specialist/doctor, please send a Cerner message to the clinic pool or to the provider if there are changes to the Asthma Action Plan or if the patient needs to be seen for a follow-up sooner than anticipated:
- Clinic Pools:
- Allergy and Asthma Clinic
- Pulmonology Clinic (Red or Green Team)
- AAIR Clinic
Identifying High Risk Asthma Patients (HRAP)
HRAP is a program created to identify patients who are high utilizers of health care for asthma and/or at high risk for mortality.
Patients qualify for HRAP if:
- ≥ 4 acute care visits (ED, Urgent Care, or admission) in the 12 months OR were admitted to the PICU for asthma
Identification of these patients in the ED/Urgent Care prior to discharge allows for appropriate follow-up, but also helps ED/UCC providers know which patients are at greater risk to return for asthma care.
The High-Risk Asthma Order-set includes:
- Clinic referral to Allergy or Pulmonology subspecialty groups for long-term care
- Social Work Consult
- Environmental Health Home Assessment Referral
Educational Point
A first-time diagnosis of asthma should be avoided in the acute care setting especially for a first-time wheezing episode. Patients may be diagnosed with “wheezing” and/or “respiratory distress” but avoid labelling a patient with a chronic diagnosis like “asthma” or “reactive airways” in the acute care setting. Close follow-up with the patient’s primary care provider for further evaluation and diagnosis is recommended.
- For children ≤3 years of age, the Asthma Predictive Index (API) is valid if there are 3 or more episodes of wheezing per year. Therefore, a first-time wheezing episode does not fulfill criteria.
Modified Asthma Predictive Index (mAPI)
- Kelly CS, Andersen CL, Pestian JP, Wenger AD, Finch AB, Strope GL, Luckstead EF. Improved outcomes for hospitalized asthmatic children using a clinical pathway. Ann Allergy Asthma Immunol. 2000 May;84(5):509-16. doi: 10.1016/S1081-1206(10)62514-8. PMID: 10831004.
- Rowe BH, Spooner C, Ducharme FM, Bretzlaff JA, Bota GW. Early emergency department treatment of acute asthma with systemic corticosteroids. Cochrane Database Syst Rev. 2001;(1):CD002178. doi: 10.1002/14651858.CD002178. PMID: 11279756.
- Qureshi F, Zaritsky A, Poirier MP. Comparative efficacy of oral dexamethasone versus oral prednisone in acute pediatric asthma. J Pediatr. 2001 Jul;139(1):20-6. doi: 10.1067/mpd.2001.115021. PMID: 11445789.
- Greenberg RA, Kerby G, Roosevelt GE. A comparison of oral dexamethasone with oral prednisone in pediatric asthma exacerbations treated in the emergency department. Clin Pediatr (Phila). 2008 Oct;47(8):817-23. doi: 10.1177/0009922808316988. Epub 2008 May 8. PMID: 18467673.
- Altamimi S, Robertson G, Jastaniah W, Davey A, Dehghani N, Chen R, Leung K, Colbourne M. Single-dose oral dexamethasone in the emergency management of children with exacerbations of mild to moderate asthma. Pediatr Emerg Care. 2006 Dec;22(12):786-93. doi: 10.1097/01.pec.0000248683.09895.08. PMID: 17198210.
- Asthma Reference Guide Home
- 1. Introduction to Asthma
- 2. Asthma Diagnosis
- 3. Asthma Presentation
- 4. Goals of Asthma Therapy and Management
- 5. Asthma Severity and Asthma Control
- 6. Asthma Outpatient Management
- 7. Treating Modifiable Risk Factors
- 8. Treating Co-Morbid Conditions
- 9. Asthma Medications
- 10. Yellow Zone Therapy Options
- 11. Allergy Immunotherapy and Biologic Therapy
- 12. Asthma Exacerbations in the Emergency Department or Urgent Care
- 13. Special Asthma Considerations for Inpatient
- 14. Asthma Management in the PICU
- 15. Respiratory Support for Asthma Exacerbation
- 16. Asthma Education Resources